
IPL FOR DRY EYE
How IPL works — and what the research
actually shows
IPL is one of the most studied in-office treatments for meibomian gland dysfunction. Here's what it does, how it does it, and what the clinical evidence says about who it helps most.
$850 IPL pathway · assessment + 4 sessions, all-inclusive · See pricing ↓
Medically Reviewed by Dr. Mark Joung B.Optom (Hons) UNSW, Grad Cert Ocular Therapeutics | Updated March 2026
HOW IPL WORKS
It starts with your tear film
IPL stands for Intense Pulsed Light. It's been used in dermatology for decades — mainly for rosacea. Around 2002, an ophthalmologist noticed that patients having facial IPL were also reporting their dry eyes got better. That observation kicked off more than 20 years of research.
Your tear film has three layers. In about 85% of dry eye cases, the problem is the oil layer — produced by tiny meibomian glands along your eyelids. When these glands get blocked, your tears evaporate too fast. No amount of drops will fix a blocked gland.
We use the E-Eye device — designed specifically for treating meibomian gland dysfunction, not a skin clinic device adapted for eyes. It targets the underlying problem through four mechanisms.
Three layers working together
Prevents evaporation
Washes and nourishes
Binds tears to the eye
THE SCIENCE OF DRY EYE RELIEF
Four ways IPL restores your oil glands
Inflamed blood vessels along your lid margin feed inflammatory chemicals to your glands. IPL energy is absorbed by haemoglobin, causing these vessels to close off — cutting inflammation at its source.
IPL reduces pro-inflammatory markers in the tear film and upregulates anti-inflammatory ones. Less inflammation means your glands can recover and start producing oil normally again.
Demodex mites in eyelash follicles worsen gland blockage and are a common driver of chronic blepharitis. IPL raises mite temperature high enough to eliminate them — 83% of patients were mite-free after 3 sessions.
There's some evidence IPL softens the thickened oil blocking your glands, making it easier to express and flow naturally. This mechanism is still debated. Supporting gland health between sessions with omega-3 supplementation may also help.
Clinical Evidence for IPL Dry Eye Treatment
What the research actually shows
This isn't a treatment built on theory or marketing claims. IPL for dry eye is supported by a substantial and growing body of research — including multiple randomised controlled trials (the gold standard in clinical evidence) and several large meta-analyses that pool data across hundreds of patients.
of patients show measurable improvement in gland function and symptoms.
improvement in tear break-up time across three separate meta-analyses.
clinical studies reviewed in the latest systematic review (2024).
adverse events reported in any published study.
THE KEY STUDIES INVOLVING IPL
Research we rely on
The first properly controlled trial using the E-Eye device — the same device we use. Twenty-eight patients, double-masked and placebo-controlled. Demonstrated significant improvements in both tear film oil quality and patient-reported symptoms.
IPL plus gland expression versus gland expression alone. Forty-five patients over 32 weeks. IPL was significantly superior across every measure — tear stability, lid margin health, and gland function.
The multi-centre, sham-controlled RCT that supported FDA approval. Significant improvement in tear stability, gland function, and expressible glands. Authors declared conflicts with Lumenis — common in device research, but worth knowing.
The most comprehensive review to date — 79 clinical studies synthesised. The authors concluded that the majority demonstrated improvements in both symptoms and clinical signs.
Most recent meta-analysis pooling data from 13 RCTs. Reported statistically significant reductions in dry eye symptom scores compared with placebo.
The research is strong — but it's not a guarantee. Every patient is different, and your results will depend on factors like how long you've had dry eye, how much gland function is still intact, and how your body responds to treatment. The evidence certainty is rated as moderate (not high) by systematic reviewers. Benefits typically require maintenance every 6–12 months. And patients with severe gland atrophy are less likely to respond well. That's why we encourage assessment sooner rather than later.
DRY EYE TREATMENT COMPARISON
How IPL compares to other options
Targets inflammation, closes abnormal vessels, clears mites, restores gland function.
79+ studies, multiple RCTs.
4 sessions, 3 months, $850 total. No downtime.
Softens blocked oil through heat.
Helpful but limited.
Free at home. IPL improves tear stability 4× more effectively.
Heats and massages glands mechanically.
Several RCTs; no head-to-head vs IPL.
Single session ~$900–1,200. IPL may be superior for tear stability.
Temporarily replaces moisture.
Symptom relief only.
Doesn't treat the cause. Fine as supplement.
Reduces ocular inflammation.
Well established.
We prescribe directly. Can complement IPL.
Anti-inflammatory antibiotic.
Moderate evidence.
Daily tablets, weeks/months. Potential GI side effects.
TRANSPARENT PRICING
Two pathways: diagnose or treat
Two pathways depending on what you actually need. The Dry Eye Test Package gets you a proper diagnosis - what’s causing your symptoms and which treatment options make sense. The IPL Treatment Pathway is the treatment itself- same diagnostic workup included, plus the full IPL course.
- Bulk-billed Medicare consultation
- NIBUT (non-invasive tear breakup time)†
- Meibography imaging*†
- Treatment recommendation
- Bulk-billed Medicare consultation
- NIBUT (non-invasive tear breakup time)†
- Meibography imaging*†
- Treatment recommendation
- 4 IPL sessions on the E-Eye device
- Progress check at each session
- Yearly review included
- Top-up sessions discussed individually
*Meibography imaging available from May 2026. †What NIBUT and meibography actually measure — see below ↓
COST IN CONTEXT
Comparable IPL courses in Sydney typically start above $1,000 — and most don't include the diagnostic workup. We've kept ours at $850 all-inclusive because it makes the right call easier when patients are weighing whether IPL is worth trying.
WHAT’S MEASURED
What’s actually in the assessment
NIBUT and meibography (or meibomiography) are two specialised tests that allow us to assess and grade dry eyes severity. Both are non-contact, quick, and painless - but neither is part of a standard eye test or covered by Medicare.
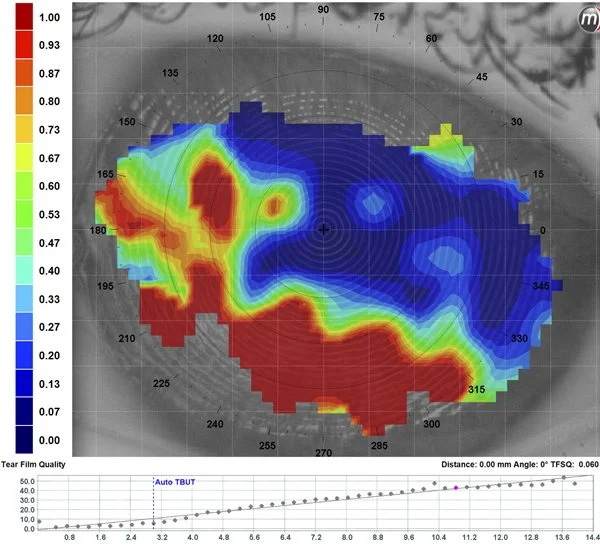
NIBUT
Non-Invasive Tear Breakup Time
Measures how long your tear film stays stable between blinks. Anything under 10 seconds suggests evaporative dry eye — usually pointing to a meibomian gland problem.
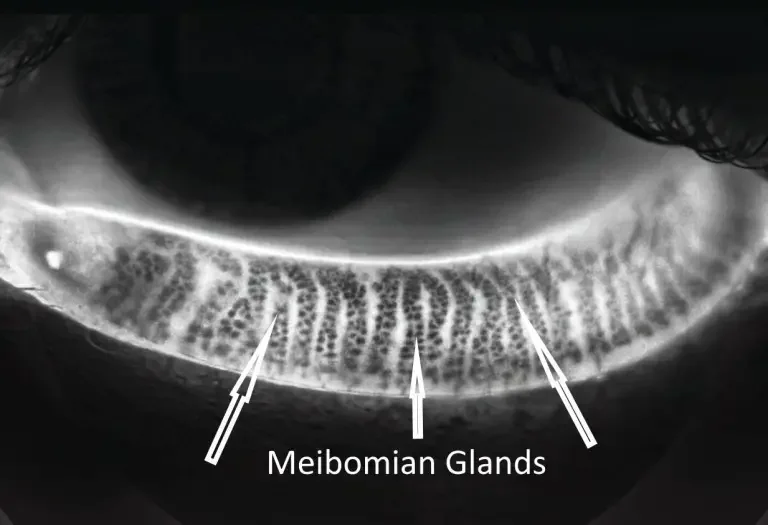
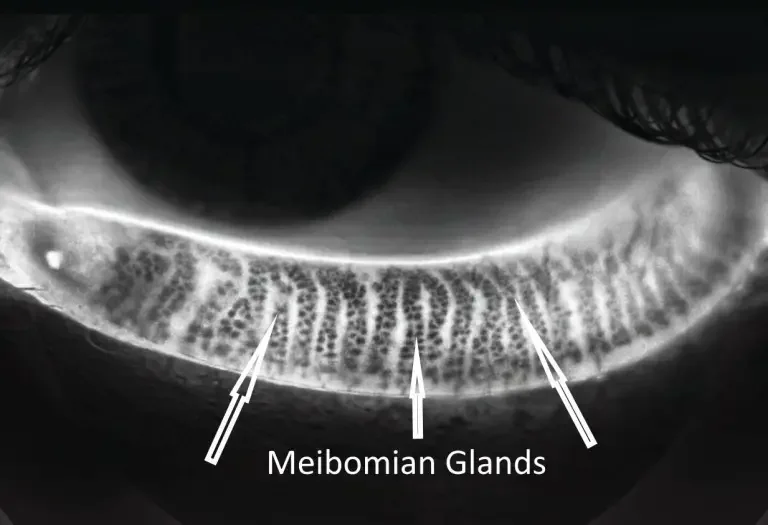
MEIBOGRAPHY
Infrared imaging of your meibomian glands
Captures the actual structure of the oil glands inside your eyelids. Shows whether they're healthy, partially atrophied, or significantly dropped out — important for staging dry eye severity and monitoring change over time.
IPL PATIENT SUITABILITY
Who responds best — and who doesn't
IPL works well for most people with meibomian gland dysfunction (MGD) — and particularly well for some. If your dry eye comes alongside rosacea or facial flushing, red or inflamed eyelid margins, Demodex-related blepharitis, or you've started losing tolerance to contact lenses as your eyes dry out, you're often a strong IPL candidate. It still isn't right for everyone, though, and being upfront about that is part of how we practise.
Are You a Good Candidate for IPL?
IPL is a highly effective, targeted medical therapy—but it isn't for everyone. Answer 4 quick questions to check your suitability.
1. How much relief do you get from standard eye drops?
2. Do your eyelids often look red, swollen, or have tiny visible blood vessels?
3. How does your skin typically react to the sun?
4. Do any of the following apply to you right now?
We don't expect you to diagnose yourself. That's what the free suitability consultation is for — we'll assess your glands and give you an honest recommendation.
OUR IPL DEVICE
The E-Eye - purpose built for dry eye

Designed specifically for meibomian gland dysfunction — not a general-purpose skin device. The pulse sequence, energy settings, and treatment protocol are all calibrated for the periocular area.
This is the same device used in the landmark Craig 2015 trial — the study that first proved IPL works for dry eye under rigorous, placebo-controlled conditions.
DURING IPL TREATMENT
What happens during a session
Each session takes about 20-30 minutes. Here’s the process:
Relax in the treatment chair.
Protective shields placed.
Coupling gel on the lids.
Gentle light, ear to ear.
20 minutes · No downtime.
Most people describe a brief warm flash — not painful.
Your skin might look slightly pink for an hour. You can drive home straight after.
THE FULL IPL COURSE
Four sessions over three months
-
Day1Session 1
First treatment. Sets the baseline.
-
Day15Session 2
Builds on the first. Some notice improvement.
-
Day45Session 3
Most patients notice a real shift here.
-
Day75Session 4
Final session. Full results assessed.
This protocol was validated in the Craig 2015 trial. Research shows at least four sessions are needed for sustained cumulative benefits. Maintenance is typically one top-up every 12 months.
FREQUENTLY ASKSED QUESTIONS
How does IPL treat dry eye?
IPL targets inflammation and abnormal blood vessels around the eyelids, which improves the function of your meibomian glands. This restores the oil layer of your tear film — the root cause of most chronic dry eye, particularly evaporative dry eye and meibomian gland dysfunction.
What does IPL cost at Concord Eyecare?
There are two pathways. If you've already decided IPL is right for you, the full IPL Treatment Pathway is $850 all-inclusive — that covers the initial assessment, NIBUT and meibography testing, 4 IPL sessions over 3 months, and ongoing reviews. If you're still working out what's going on with your eyes, the Dry Eye Test Package is $50 on top of a bulk-billed Medicare consultation and includes the same diagnostic workup without committing to IPL.
How many IPL sessions do I need?
Most patients need 4 initial sessions spaced 2–4 weeks apart, followed by maintenance sessions every 6–12 months. Results are cumulative — each session builds on the last, and the Craig 2015 RCT validated this 4-session protocol.
Is IPL for dry eye painful?
Most patients describe it as a warm flash with a brief tapping sensation. It's not painful. Each session takes about 20 minutes and you can drive home and return to normal activities straight after. Your skin might look slightly pink for an hour.
Is IPL covered by Medicare or private health insurance?
IPL for dry eye is not covered by Medicare. Most private health funds don't rebate it either, though a small number pay a partial rebate under therapy or dry eye benefits — we check your specific fund at the assessment so you know before committing. The initial dry eye consultation is bulk-billed; the $50 Test Package and the $850 IPL Pathway are both private fees.
Who is suitable for IPL dry eye treatment?
IPL works best for evaporative dry eye caused by meibomian gland dysfunction. It's not suitable for very dark skin types (Fitzpatrick V–VI), people on photosensitising medications (such as certain acne or antibiotic treatments), those who are pregnant, or those with active facial conditions. We assess all of this during the suitability consultation.
How is IPL different from warm compresses or LipiFlow?
Warm compresses soften blocked oil through heat — helpful but limited. LipiFlow physically expresses the glands in a single 12-minute treatment. IPL works at the inflammation level, addressing the cause rather than just the symptom, and the evidence base is broader. Our comparison table earlier on this page breaks down each option.
Can an optometrist perform IPL?
Yes — therapeutically endorsed optometrists in Australia can perform IPL for dry eye. All three optometrists at Concord Eyecare are therapeutically endorsed, which means we can prescribe ocular medications directly without needing a GP referral.
Key References
- Craig JP, Chen YH, Turnbull PRK. Prospective trial of intense pulsed light for the treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 2015;56(3):1965-1970.
- Toyos RT, McGill JB, Briscoe D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction. Photomedicine and Laser Surgery. 2015;33(1):41-46.
- Liu R, Rong B, Tu P, et al. Analysis of cytokine levels in tears and clinical correlations after intense pulsed light treating meibomian gland dysfunction. Am J Ophthalmol. 2017;183:81-90.
- Arita R, Fukuoka S, Morishige N. Multicenter study of intense pulsed light therapy for patients with refractory meibomian gland dysfunction. Cornea. 2018;37(12):1566-1571.
- Toyos R, Desai NR, Toyos M, Dell SJ. Intense pulsed light for meibomian gland dysfunction: sham-controlled multicenter randomised trial. PLOS ONE. 2022;17(10):e0275979.
- Xie X, Zhang Z, Zhao X, et al. Intense pulsed light therapy for meibomian gland dysfunction: systematic review and meta-analysis. Medicine. 2022;101(26):e29529.
- Fineide F, Arita R, Utheim TP. The role of intense pulsed light in the treatment of dry eye disease: a narrative review. Acta Ophthalmologica. 2024;102(2):e154-e170.
- Peira SL, Lombardo C, De Angelis P, et al. Intense pulsed light for meibomian gland dysfunction: systematic review and meta-analysis. Acta Ophthalmologica. 2025;103(1):e103-e118.
Book a free IPL suitability consultation.
15–20 minutes. We'll assess your dry eye, examine your glands, and tell you honestly whether IPL is the right option. No charge, no obligation.
DRY EYE TREATMENT HUB
Want to start from the beginning?
If you haven't read our main dry eye page yet — start there for the full overview, pricing, symptom checklist, and treatment journey.