
OVERNIGHT MYOPIA CONTROL · SYDNEY
Ortho-K Sydney — Overnight Lenses That Slow Myopia and Correct Vision
Custom overnight lenses that correct your child's vision and slow myopia progression by 50–60%. From $1,600 for two years, all-inclusive.
Reviewed by Dr Mark Joung — B.Optom (Hons) UNSW, Grad Cert Ocular Therapeutics | 800+ Ortho-K lenses fitted | Updated May 2026
WHAT IS ORTHO-K?
Corneal reshaping lenses that correct vision while you sleep
Ortho-K lenses work by applying gentle pressure to the front surface of the eye (the cornea) while your child sleeps. By morning, the cornea holds its new shape — correcting short-sightedness for the full day. The effect is temporary: stop wearing the lenses and the cornea returns to its original shape within about 72 hours. That's part of what makes ortho-K so appealing to parents — it's completely reversible.
But corneal reshaping isn't just about clear daytime vision. The lens also changes how light focuses on the peripheral retina, which signals the eye to slow down the elongation that drives myopia progression. That's the part we care about most — not just helping your child see today, but reducing how short-sighted they become over the next five to ten years.
The treatment has been used clinically since the 1960s, with modern accelerated lens designs available since the early 2000s. It's one of the most-studied myopia control treatments available, with over two decades of peer-reviewed evidence supporting both its vision correction and myopia-slowing effects.
If you're not sure what myopia is or why progression matters, our guide to myopia explains the basics.
HOW DOES ORTHO-K WORK?
The overnight cycle — and what the research actually shows
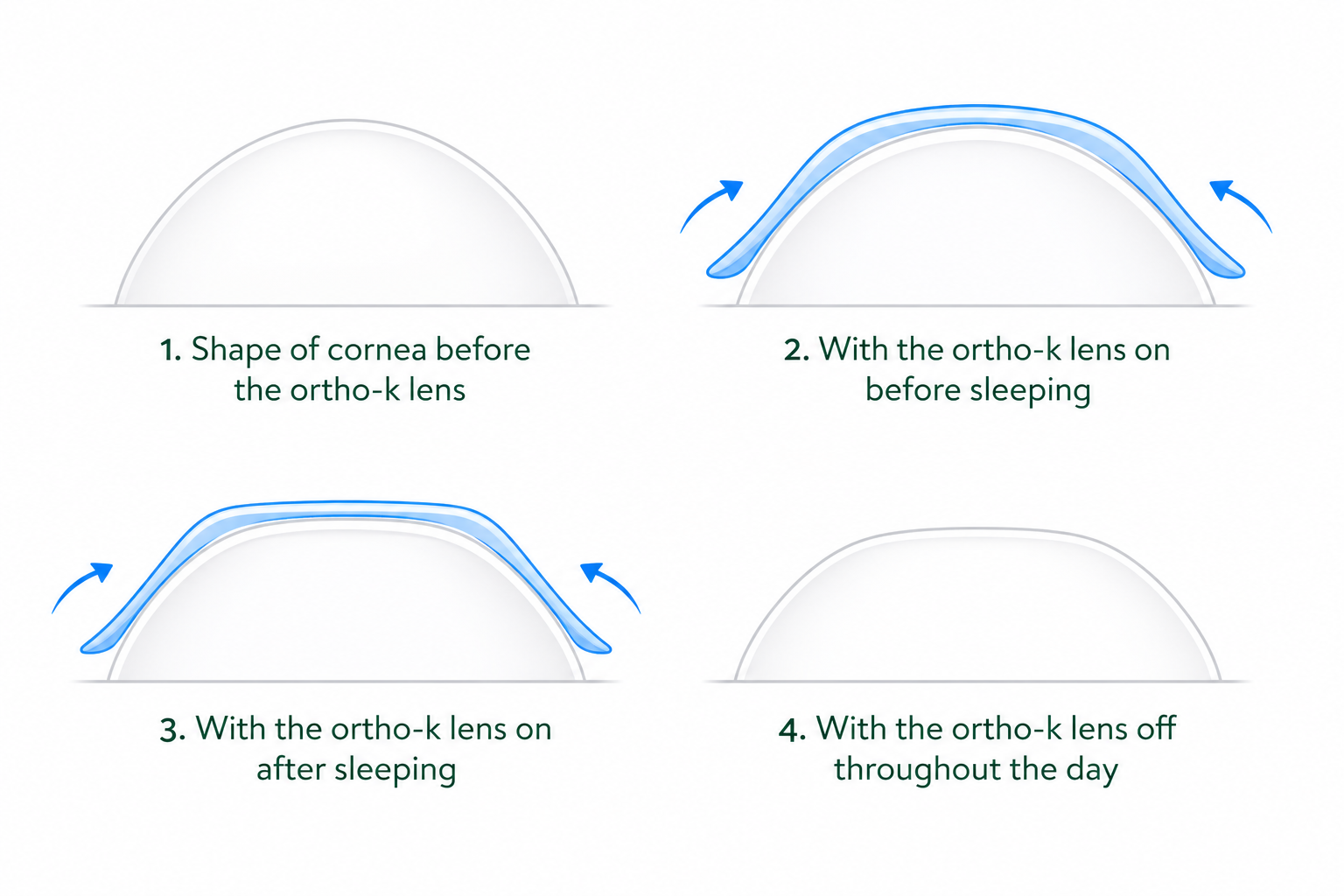
What happens overnight
The ortho-K lens sits on a thin layer of tears on the eye's surface. The lens shape — custom-designed from your child's corneal topography map — applies controlled hydraulic force that gently redistributes the epithelial layer of the cornea. The central cornea flattens by around 20–40 microns (a fraction of the thickness of a human hair), correcting the refractive error that causes blurred distance vision.
By morning, the cornea holds that new shape. Your child removes the lenses, and their vision stays clear through the day — typically 6/6 (equivalent to 20/20), sometimes 6/7.5 depending on the prescription.
The myopia control effect
The vision correction alone would make ortho-K useful, but it's the myopia control effect that makes it important for children. Because the lens changes the curvature profile of the cornea — not just the centre — it alters how light falls on the peripheral retina. Research suggests this peripheral defocus signal tells the eye to slow its axial growth, which is the underlying driver of myopia progression.
A landmark toric ortho-K trial (the TO-SEE study) demonstrated up to 63% slowing of myopia progression compared to children in standard glasses. A 2016 network meta-analysis ranked ortho-K among the top three most effective myopia control treatments alongside high-dose atropine and combination therapy. Across multiple studies, the average slowing effect is approximately 50–60% (IMI Reports, Chen/Cheung/Cho 2013).
What we actually see in our practice
Published studies are one thing. What we see in practice is a range.
There's sometimes a clinical trade-off we discuss with parents: a smaller, tighter treatment zone on the cornea provides a stronger myopia control signal, but can reduce best-corrected visual acuity slightly — to around 6/7.5 instead of 6/6. We tailor this balance based on your child's prescription, progression rate, and daily visual demands. It's the kind of decision that benefits from having fitted hundreds of lenses across a wide range of prescriptions.
Most children respond well to ortho-K alone. But some keep progressing despite good lens compliance and a well-fitted lens. When progression exceeds -0.75 dioptres per year despite treatment, we don't just stay the course — we add low-dose atropine eye drops to the regimen. Current clinical guidelines favour early, aggressive intervention, particularly for younger children where the growth window is longest.
Why slowing progression matters
Every additional dioptre of myopia your child develops increases their lifetime risk of serious eye conditions — myopic maculopathy, retinal detachment, glaucoma, and early cataract. These risks scale with how short-sighted someone becomes over a lifetime, not just their prescription at any single age. Slowing progression during childhood changes that trajectory, sometimes dramatically.
WHO IS ORTHO-K RIGHT FOR?
Children from age 6, adults who want glasses-free days
Children and teens
Most of our patients start at ages 7–8, when myopia typically accelerates. We've fitted as young as 6 — though at that age we often start with MiyoSmart first.
Adults
Vision correction only — the eye has stopped growing. Wear overnight, see clearly all day without glasses or daytime contacts.
Who it's not for
Not sure which option suits your child? We walk through every option — ortho-K, MiyoSmart, MiSight, or atropine — at a myopia control consultation.
When ortho-K isn't our first choice
We don't fit every child who walks in
Ortho-K is one of four myopia treatments we offer — not a default. For some children we'll recommend starting elsewhere, and we'll tell you that at the first consult rather than fitting overnight lenses for the sake of it. Here's when ortho-K usually isn't where we begin.
Very young children
At age 6, we'll often start with MiyoSmart spectacle lenses and move to ortho-K later — once your child is confident handling a contact lens themselves.
Families who prefer glasses
If your child isn't keen on putting anything in their eye, MiyoSmart gives a comparable level of myopia control with nothing but a pair of glasses.
Not ready for nightly lens care
Ortho-K only works if the lenses go in every night. If that's a nightly battle right now, we'll start with an option that doesn't depend on it.
Prescription or cornea outside the range
Above roughly -6.00D, or with an irregular cornea, ortho-K may not give a full day's correction. We'll walk through MiSight, MiyoSmart, or atropine instead.
And even when ortho-K is the right call, some children's corneas reshape more slowly than others. We set that expectation at the start rather than promising instant results — and adjust the lens design to get the strongest response we can for your child.
THE ORTHO-K FITTING PROCESS
From first consult to clear morning vision
Initial assessment
We map your child's cornea using a Medmont corneal topographer and check their full prescription, eye health, and suitability for ortho-K. This appointment takes about 45 minutes. The eye test component is bulk-billed where eligible.
Lens fitting & teaching
Custom lenses arrive approximately one week after the assessment. We teach your child (and you) how to insert and remove the lenses safely. This session takes 30–45 minutes — we don't rush it, because confident handling from the start makes the whole process smoother.
Morning teleconsult
The morning after the first night of wear, we check in by phone or video. How was the night? How's the vision this morning? This early touchpoint catches any comfort or fit issues immediately.
First in-practice review
We compare corneal topography maps to the baseline to see exactly how the reshaping is progressing. Most children are seeing significantly clearer by now — we check the fit and make any lens adjustments needed.
Progress review
By one month, most children have stable daytime vision. We confirm the reshaping is on target, check eye health, and make sure the care routine is working well at home.
Settling review
Final check before moving to routine care. We confirm the prescription correction is holding, the cornea is healthy, and the treatment is doing its job. From here, reviews move to every six months.
Six-monthly routine reviews
At each six-monthly review, we measure axial length using IOLMaster 500 biometry — the most objective way to track whether myopia control is working, because it measures the actual length of the eye rather than relying on prescription changes alone.
If any issues arise at any stage, the review schedule resets. We don't skip ahead — we bring your child back in, assess the problem, adjust the lens or routine as needed, and restart the monitoring sequence from that point.
Ready to find out if ortho-K is right for your child?
Book a Myopia Assessmentor call (02) 8765 9600
ORTHO-K PRICING
Three tiers based on your child's prescription — from $1,600
First two years — all-inclusive
| Tier | Price | Typical patient |
|---|---|---|
| Standard | $1,600 | Mild to moderate myopia, standard corneal shape |
| Advanced | $1,900 | Higher prescription or mild astigmatism |
| Complex / toric | $2,200 | High myopia, significant astigmatism, complex corneal shape |
Each tier includes: custom-designed lenses, all fitting appointments, lens insertion and removal teaching, scheduled follow-up reviews through Year 2, and any lens replacements needed within the package period.
Year 3 onwards — maintenance packages
| Tier | Price (per 2-year package) |
|---|---|
| Standard maintenance | $1,000 |
| Advanced maintenance | $1,200 |
| Complex maintenance | $1,500 |
Maintenance packages cover replacement lenses (children's prescriptions change as they grow), all review appointments, and ongoing axial length monitoring.
Health fund rebates
Most private health funds with optical extras provide a rebate toward ortho-K lenses. The amount varies by fund and cover level — we recommend checking with your fund before the fitting appointment. We process claims on the spot with HICAPS.
We publish our pricing because we believe parents should be able to compare costs before booking. For a detailed year-by-year breakdown — including how ortho-K compares to the total cost of glasses, soft contact lenses, and other myopia control options over your child's growing years — see our complete ortho-K cost guide.
ORTHO-K VS OTHER MYOPIA TREATMENTS
How overnight lenses compare to MiyoSmart, MiSight, and atropine
| Factor | Ortho-K | MiyoSmart | MiSight | Atropine |
|---|---|---|---|---|
| Type | Overnight rigid lens | Spectacle lens (DIMS) | Daily soft contact lens | Eye drops |
| Efficacy | 50–60% | ~60% | 59% | Up to 50% |
| Wear schedule | Nightly (removed AM) | All-day glasses | Daytime contact lens | Nightly drop |
| Corrects vision? | Yes — no daytime correction | Yes (glasses) | Yes (contacts) | No — needs glasses/contacts |
| Typical age | 7+ | 6+ | 8–12 (FDA) | Any |
| Starting cost (CEC) | From $1,600 / 2 yrs | From $600 / pair | Subscription | Drops + consult |
Efficacy: ortho-K (IMI Reports, Chen/Cheung/Cho 2013), MiyoSmart (Lam et al., HOYA), MiSight (CooperVision FDA trial), atropine (LAMP study). Figures represent average slowing of myopia progression vs standard correction.
We fit all four treatment options at Concord Eyecare. There is no single "best" treatment — the right choice depends on the child.
How we decide in clinic
Atropine drops can be used alone or added to any of the lens-based treatments when progression is faster than expected.
Further reading
WHY FAMILIES CHOOSE CONCORD EYECARE FOR ORTHO-K
800+ lenses fitted — and the clinical depth to back it
We've been fitting ortho-K for over a decade — 800+ lenses and counting. That volume matters because it means we've seen the edge cases: the kids who don't adapt quickly, the fits that need three rounds of refinement, the prescriptions at the upper end of suitability. Experience with the outliers is what makes the standard cases straightforward.
Ortho-K is not a side offering here — it's a core focus alongside our complete myopia control toolkit. We fit ortho-K, MiyoSmart, MiSight, and prescribe atropine, so the recommendation is always based on what suits your child, not what we happen to offer.
B.Optom (Hons) UNSW · Grad Cert Ocular Therapeutics · Advanced Paediatric Eye Care (UNSW) · One of the first Australian optometrists to fit MiyoSmart · 800+ ortho-K lenses fitted
Dr Nikki Peng
B.Optom (Hons 1st Class) UNSW · Grad Cert Ocular Therapeutics · Published dry eye author
Dr Vivian Li
B.Optom (Hons) UNSW · Grad Cert Ocular Therapeutics · ACBO Advanced Children's Vision Certificate (ACBO Prize)
All three optometrists are therapeutically endorsed — qualified to diagnose and treat eye conditions, not just prescribe lenses.
What Ortho-K families say
"Mark was patient, kind, and professional, making her feel comfortable throughout the visit. We truly appreciate the clear explanations and the time taken to ensure she received the best care."
"I take my two kids here. My experience is that they are always very professional, with a lot of care and patience. Especially for my son who has just been fitted with OrthoK lenses. The after care service has been exceptional."
"I've always travelled to see Dr Mark. He was especially patient in helping my children transition into orthok, really took his time explaining and easing their anxiety. Big thank you for Dr Mark."
ORTHO-K QUESTIONS ANSWERED
Common questions from parents considering ortho-K
Is ortho k safe for children?
Yes. Ortho-K has been used clinically for decades, with a safety profile comparable to other forms of contact lens wear. The main risk is infection — preventable with proper lens hygiene. We teach every family a clear care routine and monitor closely at follow-up visits. Read more about ortho-K safety.
How old does my child need to be?
Most of our ortho k patients start between ages 7 and 8. We've fitted children as young as 6, though at that age we often begin with MiyoSmart spectacle lenses and transition to ortho-K once the child is comfortable handling contact lenses. There's no upper age limit.
How quickly will my child see results?
Most children achieve clear daytime vision within one to two weeks. Higher prescriptions can take four to six weeks. There's often 10–20% clarity variance by end of day during the first week or two — this settles as the cornea adapts.
Can my child play sport with ortho k lenses?
Yes — that's one of the biggest advantages. Because the lenses are only worn at night, there's nothing on the eyes during the day. No glasses to worry about during contact sport, no lenses to lose in the pool.
What happens if we stop ortho k?
The effect is fully reversible. The cornea returns to its original shape within approximately 72 hours and vision goes back to where it was. The myopia control effect also stops — progression resumes at its natural rate.
How much does ortho k cost?
From $1,600 for the first two years, covering custom lenses, all appointments, and reviews. We offer three tiers based on prescription complexity. See the full cost breakdown.
Can we claim ortho k on health insurance?
Most private health funds with optical extras provide a rebate toward ortho-K lenses. The amount varies by fund and cover level. We process claims on the spot with HICAPS.
Can ortho k be combined with atropine?
Yes — combination therapy is common for fast progressors. When progression exceeds -0.75 dioptres per year, we typically add low-dose atropine drops — including the newer Eikance formulation — to strengthen the effect.
Does ortho-K work for astigmatism?
Yes — for regular astigmatism, we fit toric ortho-K designs that correct both myopia and astigmatism together (complex tier, from $2,200 for two years). Irregular astigmatism — the kind seen with conditions like keratoconus — generally isn't suitable for ortho-K, and we'd talk through other options. We confirm which type you have at the initial appointment.
ORTHO-K CLINICAL REFERENCES
- Chen C, Cheung SW, Cho P. Myopia control using toric orthokeratology (TO-SEE study). Invest Ophthalmol Vis Sci. 2013;54(10):6510-6517.
- Lam CSY, Tang WC, Tse DY, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br J Ophthalmol. 2020;104(3):363-368.
- Yam JC, Jiang Y, Tang SM, et al. Low-Concentration Atropine for Myopia Progression (LAMP) study. Ophthalmology. 2019;126(1):113-124.
- Chamberlain P, Peixoto-de-Matos SC, Logan NS, et al. A 3-year randomized clinical trial of MiSight lenses for myopia control. Optom Vis Sci. 2019;96(8):556-567.
- International Myopia Institute. IMI Report on Interventions for Myopia Onset and Progression. Invest Ophthalmol Vis Sci. 2019;60(3):M106-M131.
- Sankaridurg P, et al. IMI Impact of Myopia. Invest Ophthalmol Vis Sci. 2021;62(5):2.
Serving Sydney families from our North Strathfield practice — 161 Concord Rd, North Strathfield NSW 2137
Ready to talk about Ortho-K?
Book a myopia control assessment with Dr Mark Joung, Dr Nikki Peng, or Dr Vivian Li. We'll check suitability, walk through all the options, and give you a clear answer on whether ortho-K is right for your child — no pressure.
Book an Ortho-K Assessmentor call (02) 8765 9600